
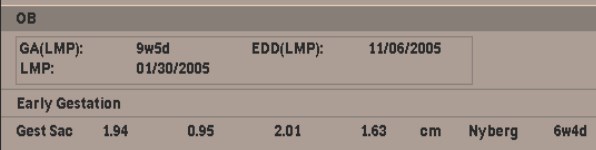
Sonography ofFirst TrimesterIntrauterine Pregnancy:Abnormal Outcomes Mindy M. Horrow, MD,FACRDirector of Body ImagingAlbert Einstein Medical CenterPhiladelphia, Pennsylvania
Estimation of Early PregnancyFailure Rates
“...nearly one third of thepregnancies detected by anelevation in the urinary -hCGlevel failed to survive to delivery.About two thirds of these lossesoccurred before the pregnancyhad been clinically recognized.”
Wilcox, NEJM 1988
Discriminatory Level for -hCG
-hCG level above which it isABNORMAL NOT to identify agestational sac
1000 mIU/mL (1st IRP) *
1700-2000 mIU/mL (1st IRP) **
Strict cut-off of 2000 mIU/mL will misssome normal IUPS ***
*Bree, AJR 1989
**Nyberg, JUM 1987
*** Mehta, Radiology 1997
When is the pregnancyabnormal for
Gestational sac without anembryo?
Gestation sac with an embryo
a. without cardiac activity?
b. with cardiac activity?
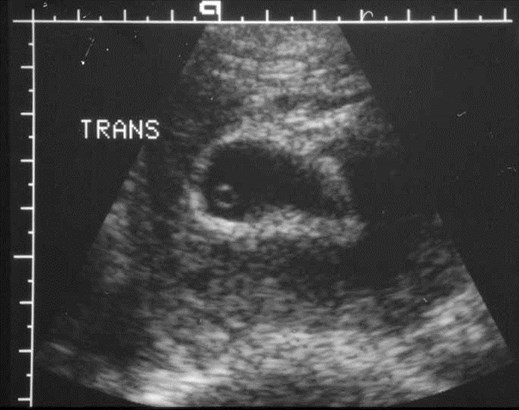
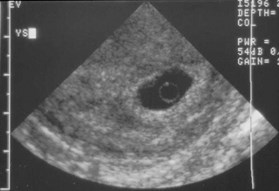
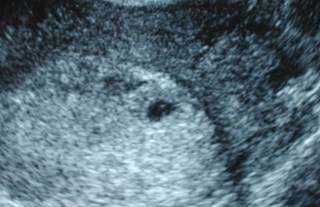
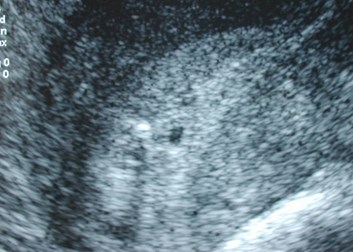
There is an intrauterine gestationalsac without an embryo. Is itnormal?
Size - without yolk sac or embryo
Ancillary characteristics: shapeposition, appearance
Slow growth
Amniotic membrane
Abnormal yolk sac - size and shape
Abnormal Appearance ofGestational Sac
Irregular contour
Thin decidual reaction (< 2 mm)
Absent double decidual sac
Low position
Normal gestational sac grows 1.13mm/day. Use this information toplan follow-up studies.
Differential diagnosis ofan empty gestational sac
Normal, early intrauterinepregnancy
Abnormal intrauterine pregnancy
Pseudosac of an ectopicpregnancy


Threatened AB
10mm empty sac
2 days later, sac
smaller, low in
position
Failed Pregnancy

Inevitable abortions


Spontaneous abortion with sac in vagina
Discriminatory Level of GestationalSac Size for Visualization of YolkSac
MSD (mm)Weeks
6-8 (13) 51/2
Levi, Radiology 1988
Bree, AJR 1989


12mm sac
with yolk sac
1 week later- minimalgrowth= failedpregnancy

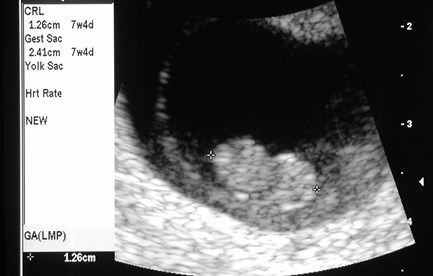
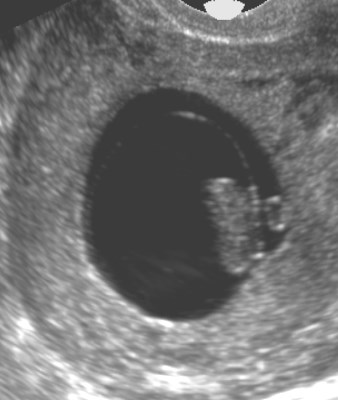
Early pregnancy
With bleeding, 3/30
Early IUP, possiblyabnormal


Follow-up, 4/8
Definitive failed pregnancy
MSD
Discriminatory Level of GestationalSac Size for Visualization ofEmbryo
MSD (mm)Weeks
10-17 (18) 61/2
Levi, Radiology 1988
Bree, AJR 1989
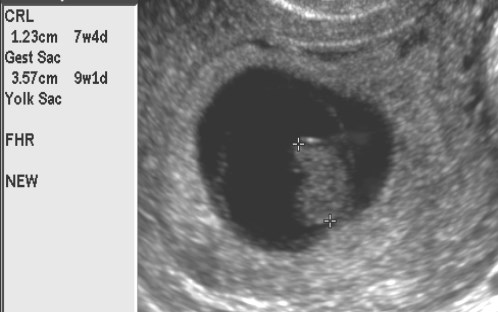
22mm MSD, no embryo = failedpregnancy
Yolk Sac and Gestational SacSize Parameters Revisited
30/135 (22%) of 8 mm sacs withoutyolk sac developed live embryos
5/59 (8%) of 16 mm sacs without anembryo developed live embryos
(N.B. used 5 MHz transducer)
Rowling, Radiology 1997
Influence of TransducerFrequency
Using 9-5 MHz probe
Threshold Discriminatory(mm)(mm)
__________________________________________________________________________
Yolk sac55
Embryo813
Rowling, AJR 1999


Mean sac diameter =6mm
5 MHz 8-4 MHz
Yolk Sac
Controversy - is absenceabnormal?
Large, small and abnormallyshaped sacs associated withspontaneous abortion and fetalanomalies
Ferrazzi, Am J Ob Gyn 1988; Kurtz, AJR 1992;Reece, Am J Ob Gyn 1988;Levi, Radiology 1990;Rowling, Radiology 1997; Stampone, JCUS 1996


Enlarged yolk sac
Two weeks later
embryonic demise

Demise at 7 weeks: calcified yolk sac
Harris Radiology 1988;166:109
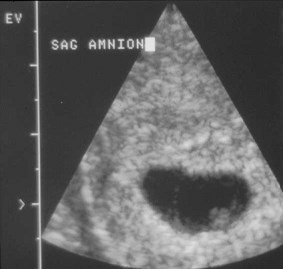
Amniotic Membrane
“Empty Amnion” - visualizationof an amnion without anembryonic pole indicates failedpregnancy
Often, amniotic membrane is toothick in cases of earlypregnancy failure
McKenna, JUM 1995

Examples of failed pregnancies:
empty amnion

Has embryonic demiseoccurred? Yes, if:
Embryo is identified with certainty
Crown rump length is greater than5 mm
No cardiac activity is detected afterat least 1 minute, preferably bymore than one observer
The study is technically adequate
Early pregnancy withbleeding
EmbryonicDemise
Negative
Pregnancy Failure Rates AfterSonographic Detection of CardiacActivity
WeeksBleedingNo BleedingOverall*
5.5 - 6 33%16%20.4%
7-910%5%7.6%
9-114%1-2%4.5%
combined data from Goldstein, Radiology 1990; Wilson, ObstetGynecol 1986; May, JUM 1991; Howe, JUM 1991, Benson,Radiology 1997
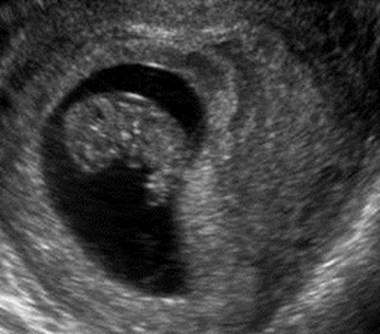
Embryo has cardiac activity.Are there signs suggesting apoor outcome?
Subchorionic hemorrhage
Bradycardia
Oligohydramnios
Polyhydramnios
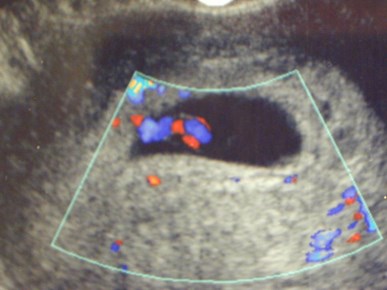
Subchorionic Collections
Presumably blood
Reported prevalence 18-50%
Associated with increased incidence ofembryonic death only if clinical bleeding
Location (placental site) may be associatedwith increased incidence of embryonic death
Dickey, Obstet Gynecol 1992; Pedersen, AJR, 1990;Kurjak, J Mat Fetal Med 1996
Subchorionic Collectionswith Bleeding
Overall spontaneous abortion rate:9.3%
Spontaneous abortion rates by size
–Small7.7%
–Moderate9.2%
–Large18.8%
Bennett, Radiology 1996


SAIUP at 7 weeks 2 days later
Large subchorionic hemorrhagewith subsequent spontaneousabortion
Subchorionic hemorrhages
Acute Subacute




Acute subchorionichemorrhage
One week later


Failure of one embryo in diamniotic-dichorionic twin pregnancy

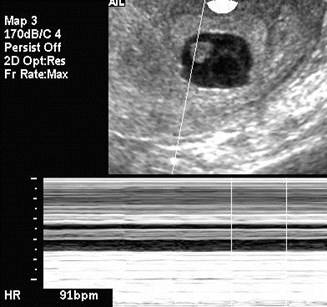
Embryonic Bradycardia
Prognosis< 6.2 weeks6.3-7.0 weeks
Dismal< 80 bpm< 100 bpm
Poor80-89 bpm100-109 bpm
Fair90-99 bpm110-119 bpm
Normal> 100 bpm> 120 bpm
Doubilet, JUM 1995
Early pregnancy with bleeding
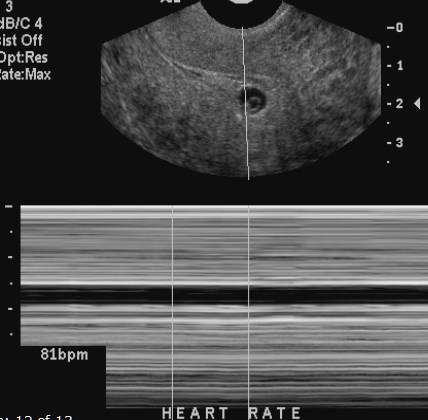
bradycardia

Failed Pregnancy
Two weeks later
Embryonic Tachycardia
> 135 bpm before 6.3 weeks
>155 bpm at 6.3 – 7.0 weeks
These pregnancies have highlikelihood of normal outcome
Doubilet, AJR 2000

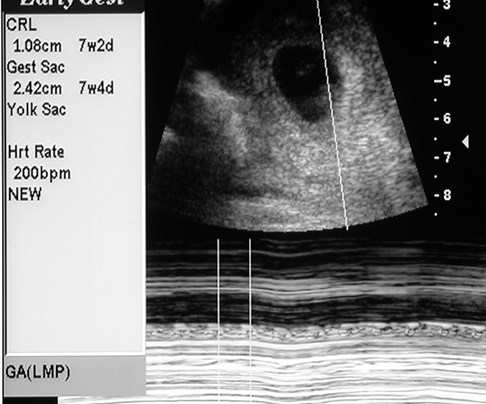
Tachycardia @ 7 weeks with normal outcome
Abnormal Outcomes withCardiac Activity
Bradycardic embryo who survivesfirst trimester has 2x risk ofanomalies
Cardiac activity seen at 6 weeks
–94% normal outcome
Cardiac activity seen at 7 weeks
–70% normal outcome
Doubilet, JUM 1999; Rosen, Fert Steril, 1990
First TrimesterOligohydramnios
MSD - CRL < 5 mm
Uncommon, < 2% of pregnancies
Increased incidence of spontaneousabortions (65-94%)
Bromley, Radiology 1991;Dickey, Obstet Gynecol 1992;Rowling, Radiology 1997




Early pregnancywith bleeding
Large amnion, oligohydramnios, abnormallyshaped yolk sac, pregnancy eventually failed.

Oligohydramnios, large yolk sac,bradycardia, eventual demise
Abnormal Amniotic Sac:first trimester polyhydramnios
Enlarged amniotic cavityrelative to CRL correlates withearly embryonic death
Increased volume of amnioticfluid may be related tocongestive heart failure
Horrow, AJR 1992; Birnholz, JUM 1995

Live 3mm embryo:large amnion &yolk sac
One week later:larger amnion, nocardiac activity


Enlarged amnion, large yolk sac, no cardiacactivity, follow-up showed spontaneous AB
Effect of Prognostic Factors onOutcome of Pregnancy withCardiac Activity
Higher pregnancy loss ratesassociated with:
–Older maternal age, assistedreproduction, symptoms ofpain/bleeding, abnormal USfindings
Effect of Prognostic Factors onOutcome of Pregnancy with CardiacActivity
Based on a stepwise logistic regressionwith gestational age as a covariate:
–“The prognosis for older mothers andfor those with assisted conception isnot statistically significantly differentfrom that for younger mothers and forthose with natural conception ifmaternal symptoms, US findings, andgestational age are the same.”
Benson, Radiology 1997
Nuchal Translucency
Sagittal (CRL) view, measured as maximalthickness of sonolucent zone betweeninner aspect of skin and outer aspect ofsoft tissue overlying the cervical spine oroccipital bone
Considered abnormal if 3mm at 13-14.9weeks gestation
Study of 10,010 patients: seen in 0.8% ofwhich 24% had abnormal karyotypes
( trisomies 13, 18, 21 and XO, triploidy)
Taipale, NEJM1997;337:1654
Nuchal Translucency
Risk of chromosomal abnormality stronglyincreased if nuchal translucency is septated
If karyotype is normal, increased incidenceof associated abnormalities: Noonansyndrome, omphalocele, duodenal atresia,muscular atrophy, hydrothorax,spontaneous abortion, infantile polycystickidneys, Joubert syndrome, hydrops
Possible mechanism: heart strain, abnormallymphatic drainage
Van Vugt Radiology1996;200:537
Reynders JUM 1997;16:101

Normal NuchalTranslucency



Diffusely increasednuchal translucency:intrauterine demise at22 weeks, Turner’sSyndrome (XO)
Endovaginal Scanning DetectsSome Anomalies in First Trimester
Fetuses (2114) scanned at 14 and 21 weeks
–Anomalies detected at 14 weeks: Focal orgeneralized edema most common, also: lowurinary tract obstructions, skeletalanomalies, CNS and CHD
–Anomalies detected at 21 weeks: ManyCHD, diaphragmatic hernia,holoprosencephaly, radial agenesis,hydronephrosis, clubfoot, cleft lip, pelvickidney
D’Ottavio, JUM 1995Bonilla-Musoles, JUM 1994
Combined First TrimesterScreening
Measurement of nuchal translucency
Biochemical Markers
–Free HCG- a metabolite of HCG with elevated levels inaneuploidy
–PAPP-A – pregnancy associated plasma protein A, low levelsassociated with aneuploidy
> 80 – 90% detection rate for major chromosomalanomalies
Non-specific marker for other non chromosomalanomalies (cardiac and syndromic)
Other US markers: hypoplastic nasal bone, abnormalblood flow of ductus venosus and tricuspidregurgitation
(Maternal age)
Universal Screening
All patients carry 2-3% risk for birth defects
Half of affected fetuses with Trisomy 21 areborn to women under 35 years of age
A screened, low risk patient at age 40 is atmuch less risk than a 20 year old who wasnot screened
With better screening options, age is nolonger as important
NT Screening requires rigorous training andquality control


Holoprosencephaly
Thickened placenta
Oligohydramnios
Triploidy
Other First TrimesterIssues
Retained products of conception
Gestational trophoblasticneoplasia
–Hydatidiform mole
–Invasive mole
–Choriocarcinoma
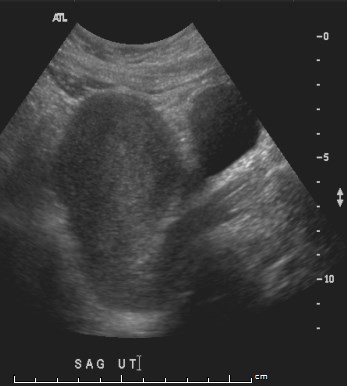
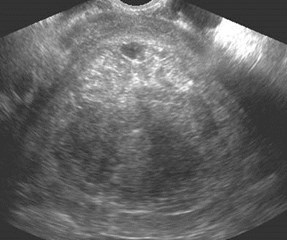
Uterine and adnexal masses
Miscellaneous
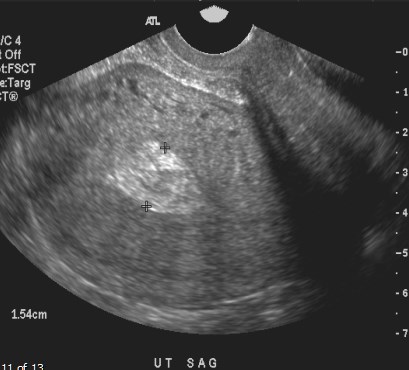
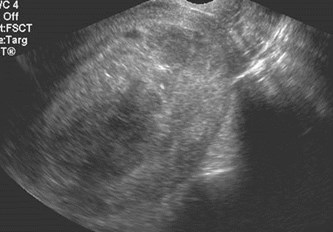
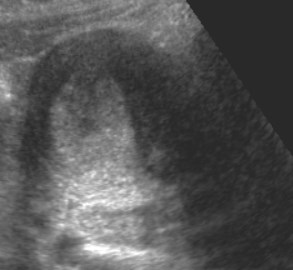
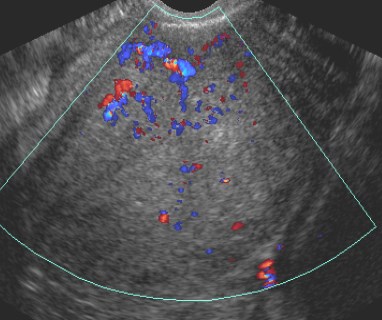
S/P therapeutic abortion one weekearlier with persistent bleeding
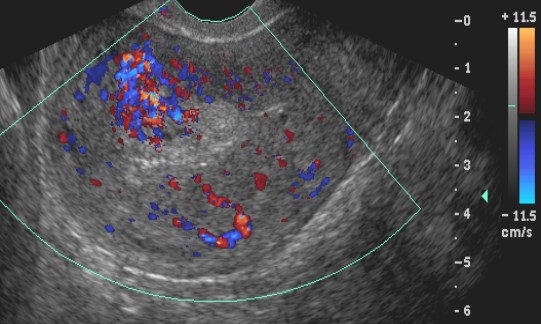
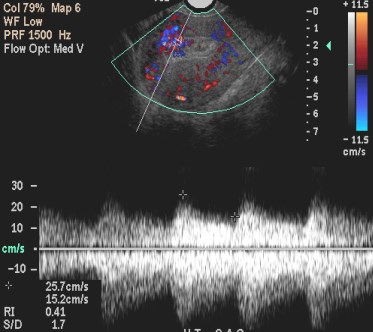
Retainedproducts ofconception
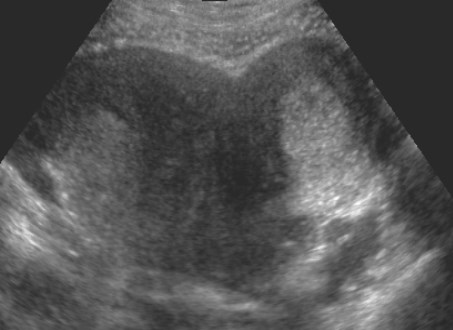
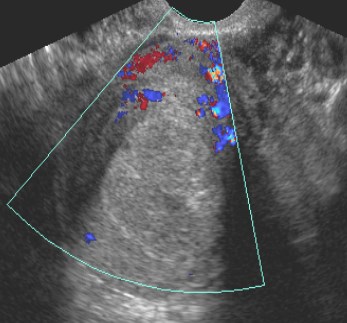
Bleeding and fever after abortion
Clinical Dx: Endometritis

Definitive 7 week IUP, patientwent for therapeutic abortion
Trv
Sag right
Sag left
3 days after abortion withnew, heavy bleeding, giveshistory of uterine anomaly
Sag R
SagL
Completed abortion right horn ofbicornuate uterus with bleeding due toshedding of decidua in smaller left horn


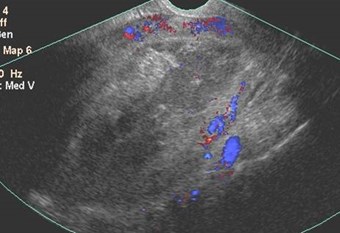
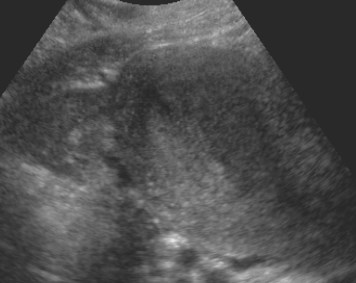
Atypical molar pregnancy- appearancesimilar to incomplete abortion
Hydatidiform Mole
Most common form of gestational trophoblasticdisease
Double, paternal chromosome
First trimester appearance variable: sac-likecollection, complex echogenic mass, thickendometrium
Only 50% correctly diagnosed prospectivelycompared to 100% of 2nd trimester molarpregnancies
Since many 1st trimester moles haveappearance of miscarriage or anembrionicpregnancy, histologic examination of tissue isimportant
Lazarus, JUM 1999;18:589
Green, Radiographics 1996;16:1371
Pregnant with bleeding
Classic appearance of MolarPregnancy
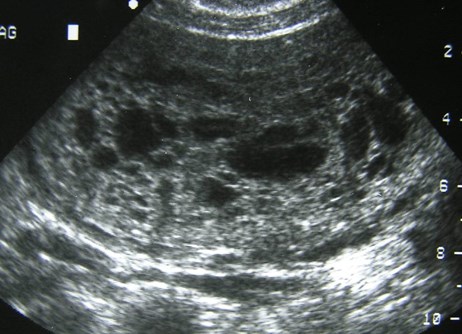
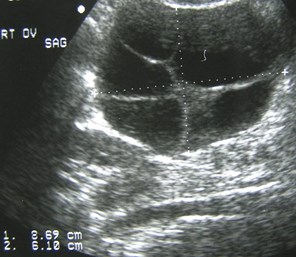
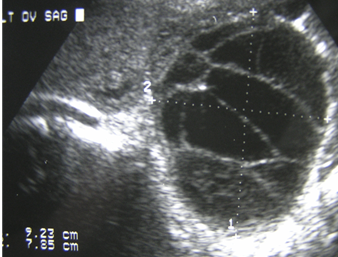
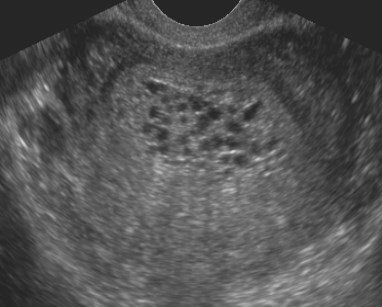
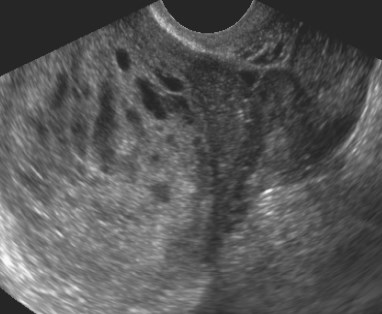
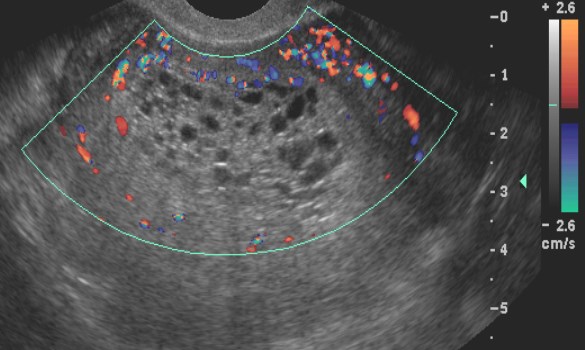
Second trimester molar pregnancywith bilateral theca lutein cysts

Early IUP and IUD
2 Days later, early IUP with smallsubchorionic hemorrhage
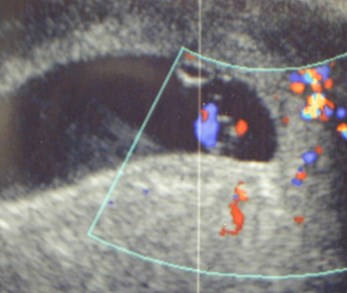
Views of umbilical cord and yolksac in an 8 week pregnancy
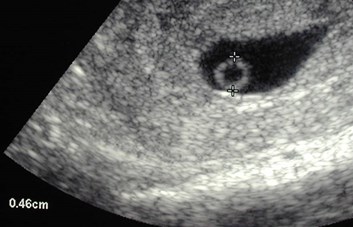
Umbilical Cord Cyst
Umbilical Cord Cysts
Occur in 3% of pregnancies
True cysts: remnants of allantois, can beassociated with hydronephrosis, patenturachus, omphalocele, Meckel’s diverticulum
False cysts (pseudocysts)- due toliquefaction of Wharton’s jelly
Impossible to differentiate true for false onUS, most resolve during 1st trimester, ifpersist into 2nd trimester there is increasedincidence of anomalies (chromosomal,omphalocele, hemangiomas)
Skibo, Radiology 1992; 182:719
Ross, Obstet Gynecol 1997;89:442


Bye-bye